Figure 20.1
Cosmetic unit bridging. A poorly designed and executed transposition flap has effaced the aesthetically important alar–cheek sulcus and also blunted t...
Figure 20.5
Motor branches of the facial nerve vulnerable in skin surgery. (—) Nerves rarely encountered; (—) nerves at risk during superficial skin surgery on th...

Figure 20.9
(a) Postoperative infection characterized by erythema, crusting and wound swelling and tenderness. (b) Areas of wound dehiscence following a flap repa...
Figure 20.13
Reverse cutting needle.
Figure 20.17
(a,b) Simple interrupted suture.
Figure 20.21
(a,b) Vertical mattress suture.
Figure 20.25
(a) This man had a basal cell carcinoma on the side of the nose; (b) this was excised and the wound was allowed to heal by second intention. (c) The c...
Figure 20.29
Bilobed flap repair on the nose. (a) A Mohs surgical defect of the right lower nasal sidewall and alar. To prevent effacement of the aesthetically cri...

Figure 20.33
Meshed split‐skin graft. (a) A split‐skin graft was harvested from the thigh skin using a power dermatome. (b) The skin was meshed on a mesher, and th...

Figure 20.37
Defects following Mohs micrographic surgery (MMS) for ‘high risk’ facial basal cell carcinoma (BCC) illustrating significant tumour extension beyond t...
Figure 20.41
Shave excision and electrosurgery of a rhinophyma. (a) This disfiguring rhinophyma was reduced in size, and (b) the nose shape recreated by shave exci...
Figure 20.45
Subfrontalis lipoma. This lipoma lies beneath the frontalis muscle. The muscle has been split vertically and is held back with forceps to reveal the l...
Figure 20.2
Arteries of the head and neck encountered in skin surgery. The labial artery lies on the inside (mucosal) surface of the lip approximately 5 mm from t...
Figure 20.6
Potential surgical hazard sites during skin surgery on the head. Nerve. (From Lawrence [ ].)

Figure 20.10
Principles of elliptical excision. The ellipse is designed to follow skin‐crease lines (a), and should be approximately three times as long as it is w...

Figure 20.14
(a–c) Tying knots with the needle‐holder.
Figure 20.18
(a,b) Buried dermal suture.
Figure 20.22
(a,b) Horizontal mattress suture.
Figure 20.26
(a) This man had a basal cell carcinoma on the temple (b) excised. (c) Three months later, the wound had healed but the scar was thick and red; (d) 15...

Figure 20.30
An interpolated paramedian forehead flap. An ill‐defined morphoeic basal cell carcinoma (BCC) of the nose. (a) Following Mohs surgical removal, an ext...
Figure 20.34
(a,b) M‐plasty design in this case prevents the scar extending onto the eyelid skin.

Figure 20.38
The stages of Mohs micrographic surgery.
Figure 20.42
Electrofulguration. Diffuse superficial coagulation can be achieved by passing the electrode of a monopolar electrosurgical unit over the skin without...
Figure 20.3
Potential surgical hazard sites during skin surgery on the head. Potential blood vessel and duct. (From Lawrence [ ].)

Figure 20.7
Nerve damage: transection of the temporal branch of the facial nerve resulting in ipsilateral paralysis of the frontalis muscle.

Figure 20.11
Scar orientation: (a) a surgical defect on the central forehead. (b) Having marked out the forehead skin rhytids, the defect is closed primarily ensur...
Figure 20.15
Surgeon's friction knot.
Figure 20.19
(a,b) Simple running sutures.
Figure 20.23
(a,b) Pulley suture.
Figure 20.27
Rotation flap for the repair of a Mohs surgical defect of the left zygomatic cheek. (a) Note the design of the flap is such that the arc of rotation p...

Figure 20.31
Complications. Flap necrosis. A large modified rhombic transposition flap on the left anterior thigh of a heavy smoker has undergone a degree of tip n...

Figure 20.35
Technique of Z‐plasty. (From Eedy et al. [ ].)

Figure 20.39
Intraoperative picture during Mohs micrographic surgery illustrating the role of the Mohs map in identifying the location of residual tumour. (a) Poor...
Figure 20.43
Electrodesiccation. Focused coagulation, e.g. of bleeding points, can be achieved with a monopolar unit using a fine‐tipped needle to deliver more con...

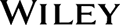
Figure 20.4
Sensory nerves on the face used in nerve block anaesthesia. Sensation on the face is served by the three main divisions of the trigeminal nerve: the o...

Figure 20.8
Vermilion approximation. (a) The vermilion border and melolabial crease have been marked prior to closure of the Mohs surgical defect. (b) Closure of ...

Figure 20.12
Shave biopsy of benign papular naevi. (a) This patient had a benign tan‐coloured naevus on the face (b) removed by shave excision followed by cautery,...

Figure 20.16
Final throw.
Figure 20.20
(a,b) Running locked sutures.
Figure 20.24
(a,b) Purse string suture.

Figure 20.28
Transposition flap. (a) A large Mohs surgical defect on the right cheek/jawline. (b) The main skin reservoir is located within the ipsilateral neck. A...

Figure 20.32
(a) Surgical defect following excision of a basal cell carcinoma. (b) A template of the defect is created on a non‐adherent dressing. (c) Template in ...
Figure 20.36
Single and multiple Z‐plasty. (a,b) Single Z‐plasty. (c,d) Multiple Z‐plasty. Note breaking up of zone of lateral tension (shaded areas) with multiple...

Figure 20.40
‘High‐risk’ facial basal cell carcinoma (BCC) suitable for Mohs micrographic surgery (MMS). (a) Extensive nasal BCC. (b) Extensive lower eyelid BCC, r...
Figure 20.44
Ring curette. (a) Curettage of a small nodular basal cell carcinoma (BCC) on the forehead using a ring curette. (b) Haemostasis with bipolar diathermy...